Almost all loss of teeth results from either caries or
periodontoclasia. These two diseases can be prevented by the
necessary personal oral hygiene. They cannot be prevented
in any other way now known. The purpose of this paper is to
present the oral hygiene procedure every person must follow in
order to entirely prevent these diseases and their consequences,
and in order to maintain the state of oral cleanliness most
people would like to maintain. The personal oral hygiene
procedure here presented as essential has evolved from practical
application of already well known fundamental information and
more recent additional pertinent information that has been
published or is in process of publication (1-4). By intensive
microscopic study of extracted teeth, employing technical
procedures (1,2,5) not usually employed for this purpose, it has
been possible to secure more accurate information regarding the
conditions at the locations and in the environment where caries
and periodontoclasia begin.
To prevent the occurrence and progress of the
lesions of these diseases their early stage must be prevented.
The oral hygiene necessary to prevent these diseases, therefore,
must effectively meet and counteract the etiological conditions
at the locations where the lesions originate.
Where Caries Begins
Enamel caries begins
principally at or about occlusal pits and fissures and at or
about the contact area between teeth. The earliest lesion
consists of a "white spot" of "chalky," partially decalcified
enamel. If the conditions are prolonged the lesion extends in
area and depth and finally this fragile, partially decalcified
enamel breaks down producing a cavity—the advanced stage of
caries. The cavity, if large enough, usually can be diagnosed by
the dentist but most of the earlier stage lesions cannot be
recognized, except upon extracted teeth.
Some idea of the frequency and extent of
these early stage lesions can be gained by very simple
procedure, even without any microscopic laboratory equipment or
experience. All that is necessary is to place extracted teeth
(preferably from persons under 20 years of age) in 10 per cent
hydrochloric acid (water 85, formalin 5, HC110) for one minute,
then wash and brush with an ordinary toothbrush to remove the
loosened cuticle, bacterial film and debris. Any "white spot,"
early stage caries lesions present can be seen satisfactorily
(Figure 1 ) with the unaided eye.
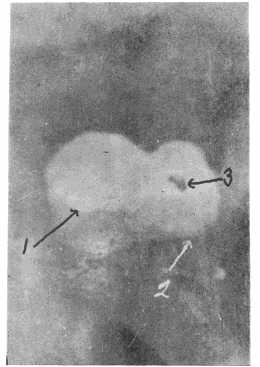 |
Fig. 1. Tooth from which the
cuticle and bacterial film were removed by
application of acid and then brushing. Note area of
"white spot" (1) chalky enamel (early stage caries)
contrasts with normal enamel. Cemento enamel
junction (2). Small cavity (3). |
They contrast well with the
more transparent normal enamel. The contrast is even sharper
after the specimen has been allowed to dry. Under magnification,
the lesions may be observed and studied better. Ordinary hand
lenses are quite helpful. The dissecting microscope is still
more helpful in studying such preparations.
It will be observed that some of these
partially decalcified areas have more or less brown stain. In
most instances these are old lesions which have been inactive
for some time, due to changes in the environment conditions
which formerly initiated the lesion and promoted activity. A
good example is proximal lesions on a tooth where the contacting
tooth was lost some time previously. Such inactive lesions are
more often found on teeth from people past 25 years of age.
Continued...
